final practical long case.
A 35yr male patient with sob,Pedal edema,Palatations.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio.
Hall ticket number : 1701006191
I've been given this case to for my final practical examination to show my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
CASE:-
- SOB since 20days
- Palpitations since 7 days
- Pedal edema since 4 days
- cough since 2 days
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 20days back then he developed sob which was insidious in onset, gradual in progressing, exertional, non seasonal, reached the present state of shortness of breath at rest(grade-4). Increases in sleeping position and relieved during sitting or standing position.
Complaint of bilateral pedal edema on and off since 4days, pitting present, extending till ankles, equal on both sides.
Complaint of cough with expectoration intermittently, not associated with fever, no diurnal variations. Expectorant- whitish to slightly pinkish in colour, non foul
smelling, no plugs, no frank blood.
There is no history of decreased urine output, no history of vomitings,loose stools etc.
PAST HISTORY:
No history of Diabetes, hypertension, CVA,CAD, tuberculosis,asthma
FAMILY HISTORY:
Not significant
No history of similar complaints in the family. No history of cardiac death in
the family.
PERSONAL HISTORY:
Diet:mixed
Appetite: normal
Sleep: Adequate
Bowel and bladder movements: regular
Alcoholic since 15yrs occasional but on continuous exposure to smoking as he was working in bar
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative to time, place and person , moderately built and moderately nourished.
Vitals:
Temperature - afebrile
Pulse rate -140 beats per min
Blood pressure- 110/70mm Hg
Respiratory rate - 40 cycles per minute
Spo2 - 98% on room air
Pallor- absent,no icterus, cyanosis, clubbing, lymphadenopathy.
Pedal edema- present, bilateral pitting type, extending till ankles.



SYSTEMIC EXAMINATION:
*CARDIOVASCULAR EXAMINATION:-
INSPECTION:
No deformity or bulge in the precordium, apical impulse seen in sixth intercoastal space 1cm lateral to the midclavicular line, no superficial engorged veins. No scars or sinuses over the skin.
No prominent pulsations in the aortic, suprasternal area, supraclavicular area. No spine deformities.
PALPATION:
Apex beat palpable in the 6th inter coastal space, left sided, 2cm lateral to the midclavicular line.
not associated with palpable thrill in the
pulmonary area.
No other palpable heart sounds, no thrill in carotid pulse, no superficial veins.
Percussion :
Right and left heart borders percussed.
AUSCULTATION:
S2 and S2 heard.
Mid diastolic murmur heard
No added sounds heard
*RESPIRATORY EXAMINATION:-
Inspection-
Chest is bilaterally symmetrical
The trachea is positioned centrally
Apical impulse is not appreciated
Chest moves normally with respiration
No dilated veins, scars or sinuses are seen
Palpation-
Trachea is felt in the midline
Chest moves equally on both sides
Apical impulse is felt in the sixth intercostal space
Tactile vocal fremitus- appreciated
Percussion-
The areas percussed include the supraclavicular, infraclavicular, mammary, axillary, infraaxillary, suprascapular, infrascapular areas.
They are all resonant.
Auscultation-
Normal vesicular breath sounds are heard.
Wheeze present in all areas.
EXAMINATION OF ABDOMEN:-
Inspection:
Skin - smooth
Shape - scaphoid
Umbilicus - normal
Abdominal wall movements - present
No visible pulsations and peristaltic movements seen.

Palpation:-
Tenderness - absent
No rise of temperature
Liver - not palpable
Spleen - mild palpable
Gall bladder - not palpable
Kidneys - not palpable
Percussion:-
Liver - dull note
Spleen - dull note
No shifting dullness, fluid thrill.
Auscultation:-
Bowel sounds heard.
No bruit.
CENTRAL NERVOUS SYSTEM EXAMINATION:-
No focal neurological deficit
*INVESTIGATIONS:
hemogram:-
Hb : 12.8
total count : 14,100
platelets : 3.93
RBC : 6.04 millions\cumm
-s.creatinine - 1.1mg\dl
- blood urea - 1.0 mg\dl
-PH : 7.43
PCo2 : 26.8 mmHg
PO2 : 76.3 mmHg
HCo3: 17.6 mmol\L
St. HCo3 : 20.4 mmol\L
TCo2 : 35
O2 stat : 94.0
LFT
total bilirubin : 2.32
direct bilirubin : 0.64
SGPT : 58
SGOT : 34
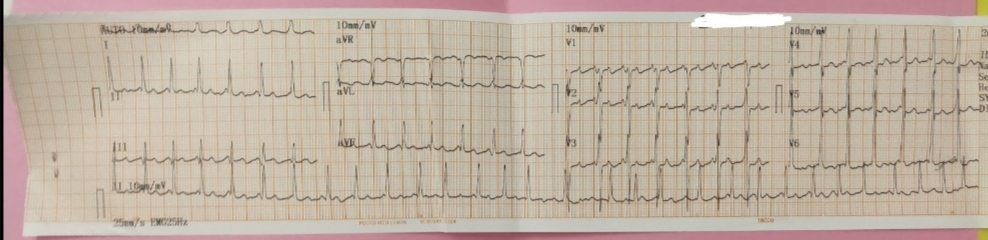
ECG-
On 8/6/22

On 09/06/22

On 12/06/22
CXR

-2D echo report:Global hypokinesia, all chambers are dilated
*PROVISIONAL DIAGNOSIS:-
•Atrial fribrilation with mitral stenosis secondary to Alcoholic dialated cardiomyopathy.
*TREATMENT:-
1)Inj.AUGMENTIN- 1.2gm Iv/BD
2)Tab.CARDARONE 150mg BD
3)Tab.AZITHROMYCIN 500mg po/OD
4)Inj.HYDROCORT 100mg iv/BD
5)Neb-IPRAVENT @10TH hrly
-BUDESERT
6)Inj.LASIX 40mg Iv/TID
7)Inj.THIAMINE 200mg in 50ml/NS/Iv/TID
8)Inj.OPTINEURIN 1amp in 50ml/NS/IV/OD
9)Fluid restriction<1.5L/day
10)Salt restriction<2g/day
11)Strict temperature charting 1hrly
Strict bp charting 2hrly.

